
Select City

Get advanced adenomyosis treatment from experienced gynaecologists at Pristyn Care. We offer personalized treatment plans, including medications, hormonal therapy, and minimally invasive laparoscopic hysterectomy for long-term relief from heavy menstrual bleeding and chronic pelvic pain.
Get advanced adenomyosis treatment from experienced gynaecologists at Pristyn Care. We offer personalized ... Read More

Free Cab Facility

No-Cost EMI

Support in Insurance Claim

1-day Hospitalization

USFDA-Approved Procedure
Choose Your City
It help us to find the best doctors near you.
Bangalore
Chennai
Coimbatore
Delhi
Hyderabad
Indore
Kolkata
Madurai
Mumbai
Noida
Pune
Thiruvananthapuram
Delhi
Hyderabad
Pune
Mumbai
Bangalore
 Pristyn Care Elantis Hospital, Lajpat Nagar, Delhi
Pristyn Care Elantis Hospital, Lajpat Nagar, Delhi
7-1-71/A/1, Dharam Karan Rd, ShivBagh, Ameerpet, Hyderabad, Telangana 500016
Pristyn Care Elantis, Ring Road, Lajpat Nagar
Pristyn Care Elantis Hospital, Lajpat Nagar, Delhi
Pristyn Care Elantis Hospital, Lajpat Nagar, Delhi
7-1-71/A/1, Dharam Karan Rd, ShivBagh, Ameerpet, Hyderabad, Telangana 500016
Pristyn Care Elantis, Ring Road, Lajpat Nagar
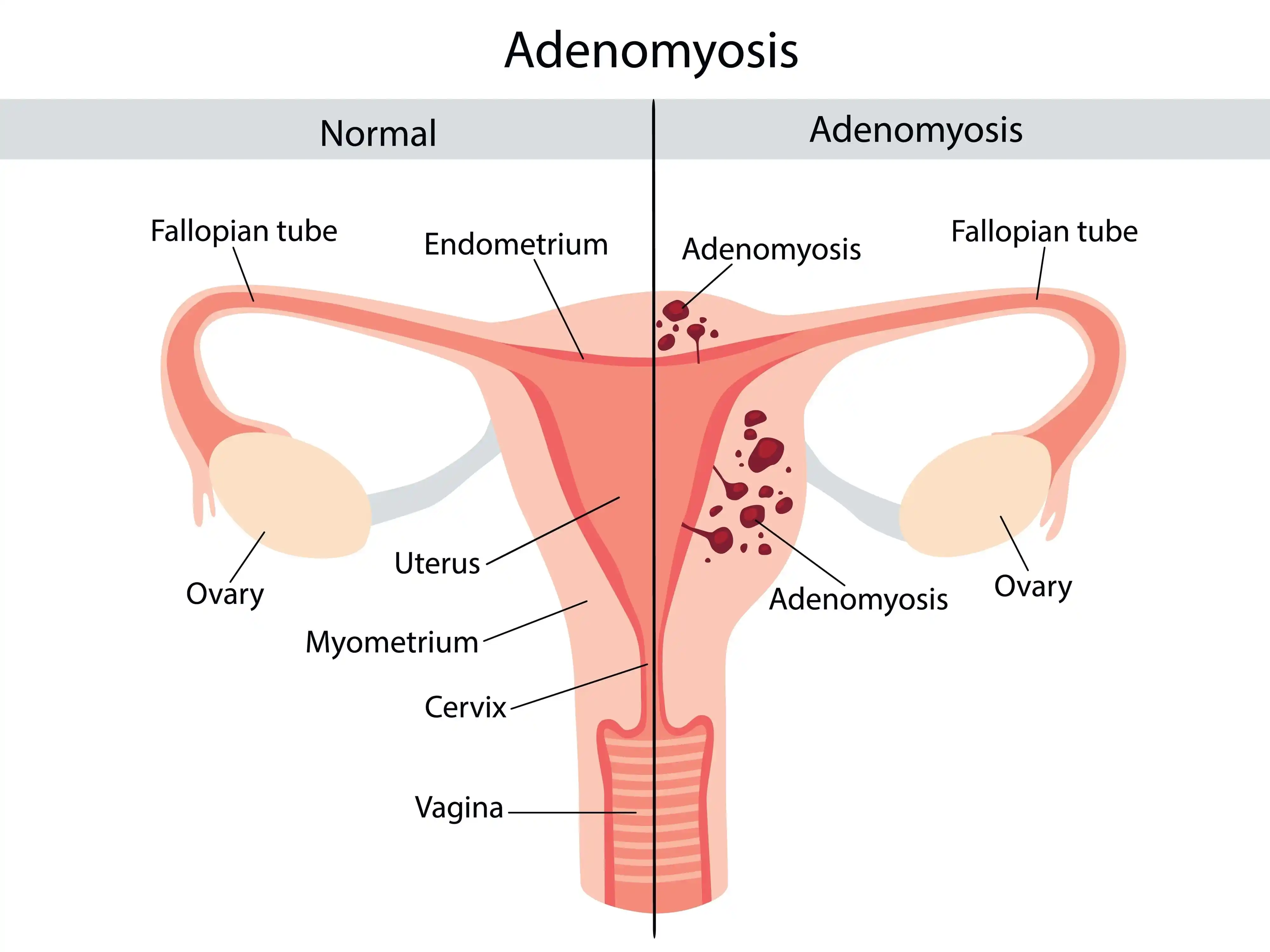
Adenomyosis is a benign uterine disorder in which the endometrial tissue grows into the muscular layer of the uterus. This abnormal growth causes the uterine muscles to become thicker and enlarged, leading to painful and heavy menstrual periods.
Unlike endometriosis, where similar tissue grows outside the uterus, adenomyosis remains confined within the uterine wall. However, both conditions can coexist in some women and may produce similar symptoms.
Although adenomyosis most commonly affects women between the ages of 35 and 50, it can also occur in younger women, particularly those who have undergone previous uterine surgery or childbirth.
Disease name
Surgery name
Duration
Treated by
Free Adenomyosis Surgery Cost Calculator
Fill details to get actual cost
Adenomyosis can vary depending on how extensively the uterine muscle is affected.
Diffuse adenomyosis occurs when endometrial tissue spreads throughout the uterine muscle. This is the most common form and often causes generalized enlargement of the uterus, heavy menstrual bleeding, severe cramps, and chronic pelvic pain.
In focal adenomyosis, the abnormal tissue is confined to a specific area of the uterine wall. Women with focal disease may experience localized pain and less severe symptoms than those with diffuse adenomyosis.
An adenomyoma is a localized mass formed by endometrial glands and uterine muscle tissue. It may resemble a uterine fibroid on imaging studies and often requires detailed evaluation to establish the correct diagnosis.
The symptoms of adenomyosis can range from mild discomfort to debilitating pelvic pain. Some women may not experience any symptoms and are diagnosed only during imaging tests or after hysterectomy.
Common symptoms include:
The severity of symptoms does not always correlate with the extent of adenomyosis. Even a small area of disease can cause significant discomfort in some women.
The exact cause of adenomyosis remains unclear. However, researchers believe that several biological and hormonal factors contribute to its development.
Possible causes include:
Although the exact mechanism is still being studied, adenomyosis is strongly influenced by female reproductive hormones and often improves naturally after menopause.
Diet & Lifestyle Consultation
Post-Surgery Recovery Follow up
FREE Cab Facility

24*7 Patient Support
Certain factors increase the likelihood of developing adenomyosis, including:
Having one or more risk factors does not necessarily mean that a woman will develop adenomyosis, but regular gynecological evaluations can help detect the condition early.
Diagnosing adenomyosis can be challenging because its symptoms often resemble those of uterine fibroids, endometriosis, or pelvic inflammatory disease. A thorough clinical evaluation and imaging tests help confirm the diagnosis and rule out other conditions.
Your gynaecologist will discuss your menstrual history, pain severity, bleeding pattern, previous pregnancies, and any prior uterine surgeries.
A pelvic examination helps assess whether the uterus is enlarged, tender, or irregular in shape, which may suggest adenomyosis.
This is the first-line imaging test for diagnosing adenomyosis. It provides detailed images of the uterus and may reveal thickening of the uterine muscle, cystic spaces, or an enlarged uterus.
Magnetic Resonance Imaging (MRI) provides highly detailed images of the uterus and is especially useful when ultrasound findings are inconclusive or when differentiating adenomyosis from fibroids.
Blood tests may be recommended to evaluate anemia caused by excessive menstrual bleeding and assess your overall health before planning treatment.
The treatment for adenomyosis depends on the severity of symptoms, the woman’s age, reproductive goals, and the extent of the disease. Women with mild symptoms may benefit from conservative treatment, while severe or persistent cases often require surgical intervention for long-term relief.
The treatment approach for adenomyosis depends on the severity of symptoms, the patient’s age, and whether she wishes to have children in the future. Women with mild to moderate symptoms can often manage the condition with non-surgical treatments aimed at reducing pain, controlling heavy menstrual bleeding, and improving quality of life.
Non-steroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen and naproxen, are commonly prescribed to relieve menstrual cramps and pelvic pain associated with adenomyosis. These medications work best when started one or two days before menstruation and continued during the menstrual cycle.
Hormonal medications help regulate menstrual cycles and reduce excessive bleeding by controlling estrogen levels. Common options include:
Although hormonal therapy can effectively manage symptoms, it does not permanently cure adenomyosis, and symptoms may return after treatment is discontinued.
Healthy lifestyle habits can help improve symptom management alongside medical treatment. Your doctor may recommend:
Women with persistent or severe symptoms despite conservative treatment may require surgical intervention.
Surgery is usually recommended when medications fail to provide adequate relief or when adenomyosis significantly affects daily life. The choice of surgery depends on the patient’s age, severity of disease, and future fertility plans.
For women who wish to preserve fertility, an adenomyomectomy may be considered in carefully selected cases. This procedure removes localized adenomyotic tissue while preserving the uterus. However, it is not suitable for all patients, particularly those with diffuse adenomyosis.
Laparoscopic hysterectomy is considered the gold-standard surgical treatment for women with severe adenomyosis who have completed their family. During this minimally invasive procedure, the uterus is removed through small keyhole incisions using a laparoscope and specialized surgical instruments.
Compared with conventional open surgery, laparoscopic hysterectomy offers:
In certain situations, such as a significantly enlarged uterus or complex pelvic anatomy, an open hysterectomy may be recommended. The surgeon removes the uterus through a larger abdominal incision. Although recovery takes longer than laparoscopic surgery, it remains a safe and effective treatment when minimally invasive surgery is not feasible.
Laparoscopic hysterectomy is performed under general anesthesia and usually takes between 60 and 120 minutes.
The procedure generally involves the following steps:
Step 1: General anesthesia is administered to ensure a painless procedure.
Step 2: Three to four small incisions are made in the abdomen.
Step 3: A laparoscope equipped with a high-definition camera is inserted to provide a magnified view of the pelvic organs.
Step 4: Specialized instruments are used to carefully separate the uterus from the surrounding tissues while preserving nearby structures whenever possible.
Step 5: The uterus is removed through the vagina or via one of the small abdominal incisions.
Step 6: The incisions are closed using absorbable sutures, and the patient is shifted to the recovery room for monitoring.
Most patients are discharged within 24 to 48 hours after surgery.
Recovery varies depending on the type of surgery performed, age, and overall health.
Typical recovery milestones include:
Following your surgeon’s postoperative instructions is essential for a smooth recovery and to minimize complications.
Ignoring persistent adenomyosis symptoms may lead to several complications, including:
Early diagnosis and timely treatment can help prevent these complications and improve long-term health outcomes.
Consult a gynaecologist if you experience:
Early diagnosis can prevent worsening symptoms and improve treatment outcomes.
The best treatment for adenomyosis depends on your age, symptoms, severity of the condition, and whether you plan to have children. Mild cases can often be managed with pain relievers, hormonal medications, or hormonal IUDs. However, women with severe pain, heavy menstrual bleeding, or an enlarged uterus may benefit from laparoscopic hysterectomy, which is considered the only permanent cure for adenomyosis.
No, adenomyosis cannot be permanently cured without surgery. Medications and hormonal therapies help control symptoms such as heavy periods and pelvic pain but do not remove the diseased uterine tissue. For women with severe symptoms who have completed their family, hysterectomy offers permanent relief.
Yes. Hysterectomy is currently the only definitive and permanent treatment for adenomyosis because it removes the affected uterus. Women who wish to preserve fertility are usually treated with medications or uterus preserving procedures to manage symptoms.
Yes. Adenomyosis may reduce fertility by affecting embryo implantation and altering the uterine environment. It may also increase the risk of miscarriage and pregnancy related complications in some women. Early diagnosis and treatment can improve reproductive outcomes for women planning pregnancy.
Adenomyosis is diagnosed through a combination of medical history, pelvic examination, transvaginal ultrasound, and MRI scan. MRI provides more detailed images and helps distinguish adenomyosis from uterine fibroids or endometriosis when the diagnosis is unclear.
Untreated adenomyosis can lead to persistent heavy menstrual bleeding, chronic pelvic pain, iron deficiency anemia, severe menstrual cramps, fatigue, and reduced quality of life. In some women, it may also contribute to fertility problems and ongoing emotional distress.
Most women recover faster after laparoscopic hysterectomy than after open surgery. Patients usually return home within 24 to 48 hours, resume desk work in about 2 to 3 weeks, and achieve complete recovery within 6 to 8 weeks by following their doctor’s post operative instructions.
Symptoms may return after stopping hormonal medications because these treatments only control the disease. However, adenomyosis does not recur after a hysterectomy since the affected uterus has been removed completely.
Adenomyosis occurs when the uterine lining grows into the muscular wall of the uterus, while endometriosis develops when similar tissue grows outside the uterus, affecting organs such as the ovaries, fallopian tubes, or pelvic lining. Although both conditions can cause painful periods and infertility, they require different treatment approaches.
You should consult a gynaecologist if you experience heavy menstrual bleeding, severe menstrual cramps, chronic pelvic pain, painful intercourse, prolonged periods, or symptoms of anemia such as fatigue and dizziness. Early evaluation allows timely treatment and helps prevent complications.

Madhu

 Recommends
Recommends
Heavy bleeding and cramps improved significantly after treatment.
Kangana
Recommends
Severe period pain reduced after treatment and cycles became manageable.
Shruti Gupta
Recommends
I feel much better after treatment
Bhawna
Recommends
Heavy bleeding and period pain reduced significantly after treatment.
Neeta
Recommends
Periods ka pain ab kaafi kam ho gaya hai.
.svg)





.svg)
.svg)









